Eating Disorders
AbdulSamad Olagunju / December 26, 2021
9 min read
Welcome to another blog post!
Quote of the Post:
"Highly organized research is guaranteed to produce nothing new." - Frank Herbert
Introduction
This term paper will briefly examine cognitive neuroscience research concerning anorexia nervosa (AN) and bulimia nervosa (BN). Eating disorders are high mortality disorders that jeopardize the well-being of an individual (Erzegovesi & Bellodi, 2016). In AN, an individual significantly reduces their caloric intake, resulting in an undernourished body. This can result in amenorrhea in women and sexual impotency in men (Erzegovesi & Bellodi, 2016, p. 305). BN is characterized by binge eating and then purging (vomiting out food). This can result in damage of the esophagus and tooth decay (Erzegovesi & Bellodi, 2016, p. 306). This paper will outline research involving executive control, visual processing, and connectivity patterns in the brains of those with AN and BN.
Bulimia Nervosa and Executive Control
This paper will begin by analyzing an experiment involving BN subjects. To understand why patients become bulimic, it is important to understand how they control their desire for food. This may reveal why they participate in over-eating and purging. A study by researchers found that subjects with BN performed worse in a task designed to measure impulsivity and regulatory control (Marsh et al., 2009). Researchers hypothesized that people with BN have disturbances in their behavioral control systems, particularly that BN patients would have less fronto-striatal regulatory circuit activation. To test this, they recruited 20 subjects who met the criteria for BN and 20 control subjects.
The subjects performed the Simon Spatial Incompatibility task. In this task, an arrow was put on a screen, and it pointed to the left or right. Moreover, the arrow would be on the left or right side of the screen. Participants had to report which direction the arrow pointed to. They did this by pressing a button. Reaction time and accuracy were measured. This experiment makes use of compatibility effects. Subjects struggled more when an arrow pointed to a direction not matching the side of the screen it was on, for example, a right arrow on the left side of the screen. An fMRI was used to perform brain imaging. Participants who made many errors, BN patients, had high activation of subcortical regions and low activation of the prefrontal cortex. Patients with more bulimic episodes had the least fronto-striatal activation (Marsh et al., 2009).
Additionally, patients with BN responded faster and made more errors than controls in more difficult situations, showing greater impulsivity (Marsh et al., 2009). This is shown in figure 1 in the appendix. These results reveal why BN patients struggle with self-control when food is involved, and this may be due to less activation in the frontal lobe (or more activation in subcortical regions). The paper also reports that their results are consistent with a previous experiment which found evidence for decreased activation of the prefrontal cortex for BN subjects as compared to controls (both were provided with stimuli of food) (Marsh et al., 2009). The prefrontal cortex plays a role in executive control, as do fronto-striatal regions of the brain. However, this study only used adult women, not allowing this data to be used to make population inferences relating to men with bulimia. Using men and more subjects with different eating disorders would have improved this study. In this study, using controls with healthy weights and eating disorders would have also revealed more about control mechanisms involving BN.
Food-Intake Regulatory Brain Circuits
In another study 77 subjects (26 with anorexia, 25 with bulimia, 26 healthy controls) had their taste and food intake regulatory brain circuits mapped (Frank et al., 2016). The researchers wanted to find out whether there were differences in the white matter connectivity of people suffering from eating disorders and healthy controls.
The food regulatory circuit in the brain involves the hypothalamus, insula, midbrain, and prefrontal/orbitofrontal cortex (Frank et al., 2016). This study used diffusion weighted imaging and an fMRI task. For brevity’s sake, we will only discuss the diffusion weighted imaging results. A computer program was used to “generate the most probable connectivity distribution,” and people with BN and AN had higher white matter connectivity between their insula and prefrontal cortex regions (Frank et al., 2016). Also, there was less connectivity between the food-intake circuit brain regions and the hypothalamus. The imaging (fig. 2) revealed that AN and BN patients had more connectivity between their insula, orbitofrontal cortex and ventral striatum.
Furthermore, participants with these eating disorders also had less connectivity between their amygdala and orbitofrontal cortex to their hypothalamus (Frank et al., 2016). This research is important because it reveals that the hypothalamus is also involved in the brain circuitry changes of those with eating disorders. AN and BN are not just due to changes in connections between the insula, orbitofrontal cortex, and ventral striatum (Frank et al., 2016). In addition, this study showed how connectivity between the middle orbitofrontal cortex and insula positively correlated the subject’s perception of sweetness in both controls and those with eating disorders, although this was related to the fMRI task that was not discussed (Frank et al., 2016).
This study could have used a larger sample size (something that many eating disorder studies struggle to obtain). In addition, anorexic patients typically also suffer from depression, and that may be a confound of this study. Nevertheless, this research highlighted the importance of hypothalamic connections in eating disorders.
Visual Processing of Food Stimuli
In the final study that will be analyzed in this paper, the brain activation of anorexic patients was measured as subjects looked at pictures of food (Santel et al., 2006). The researchers decided to perform this experiment, as hungry anorexic patients perform similarly to healthy controls who are not hungry when performing memory tasks involving food words (Santel et al., 2006). Thus, if anorexic patients have control mechanisms that allow them to feel the same way as healthy controls even when they are hungry, this may be due to altered frontal lobe control mechanisms. In addition, other research has show patients with eating disorders have less activation of their occipital cortex and inferior parietal lobe as compared to healthy controls, and interestingly enough, anorexic patients have more activation of their medial prefrontal cortex (Santel et al., 2006). In these previous experiments, there was no separation between the brain activation patterns of when subjects were hungry or full, unlike the current experiment.
This experiment wishes to ascertain the brain activation patterns of anorexic subjects when they are hungry and when they are full (Santel et al., 2006). 13 anorexic subjects and 10 healthy controls were selected (all female). When anorexia patients were full, they had less parietal cortex activation to food stimuli (images) than controls. Hungry anorexia subjects showed less activation of their occipital cortex than hungry controls. The researchers stated this was due to anorexic patients focusing less attention to food stimuli when they were hungry, compared to controls. This allows people with anorexia to resist eating even when they are hungry.
This study also found different results to other studies, as there was no increased activation of the frontal lobe in response to food stimuli in patients with anorexia nervosa (Santel et al., 2006). This result is not the same as what was seen in the first study that was reviewed (our eating disorder group had increased fronto-striatal activation). However, as this involved patients with bulimia, that may be the reason. This research, by showing pictures to both hungry and satiated anorexic/control subjects (fig. 3) was able to learn about how anorexic patients deal with their continual state of hunger as compared to healthy controls.
However, in this study, some of the anorexia patients were on anti-depressive medication, highlighting how anorexia patients often have depression. This is similar to a problem in the second study. This may have had an effect on the fMRI results. In addition, this study did not look at how the visual processing system of anorexia patients will deal with high and low-calorie foods, which is a possible avenue in the future.
Conclusion
These studies show how eating disorders reflect problems with executive control and visual processing in the brain. We learn that eating disorder patients are more impulsive in some situations and show greater executive control in others. They also process visual stimuli differently, and their connectivity in regions involving the hypothalamus is also different compared to health controls. However, these studies need better sampling (as anorexia has high comorbidity with depression) and more sample sizes so that the evidence is more conclusive.
References
- Erzegovesi, S., & Bellodi, L. (2016). Eating disorders. CNS Spectrums, 21(4), 304–309. Link
- Frank G. K. (2021). From Desire to Dread-A Neurocircuitry Based Model for Food Avoidance in Anorexia Nervosa. Journal of Clinical Medicine, 10(11), 2228. Link
- Frank, G. K., Shott, M. E., & DeGuzman, M. C. (2019). The Neurobiology of Eating Disorders. Child and Adolescent Psychiatric Clinics of North America, 28(4), 629–640. Link
- Frank, G. K., Shott, M. E., Riederer, J., & Pryor, T. L. (2016). Altered structural and effective connectivity in anorexia and bulimia nervosa in circuits that regulate energy and reward homeostasis. Translational Psychiatry, 6(11), 932. Link
- Klein, D. A., Schebendach, J. E., Brown, A. J., Smith, G. P., & Walsh, B. T. (2009). Modified sham feeding of sweet solutions in women with and without bulimia nervosa. Physiology & Behavior, 96(1), 44–50. Link
- Marsh, R., Steinglass, J. E., Gerber, A. J., Graziano O'Leary, K., Wang, Z., Murphy, D., Walsh, B. T., & Peterson, B. S. (2009). Deficient activity in the neural systems that mediate self-regulatory control in bulimia nervosa. Archives of General Psychiatry, 66(1), 51–63. Link
- Santel, S., Baving, L., Krauel, K., Münte, T. F., & Rotte, M. (2006). Hunger and satiety in anorexia nervosa: fMRI during cognitive processing of Food Pictures. Brain Research, 1114(1), 138–148. Link
- Steinglass, J. E., Berner, L. A., & Attia, E. (2019). Cognitive Neuroscience of Eating Disorders. The Psychiatric Clinics of North America, 42(1), 75–91. Link
Appendix
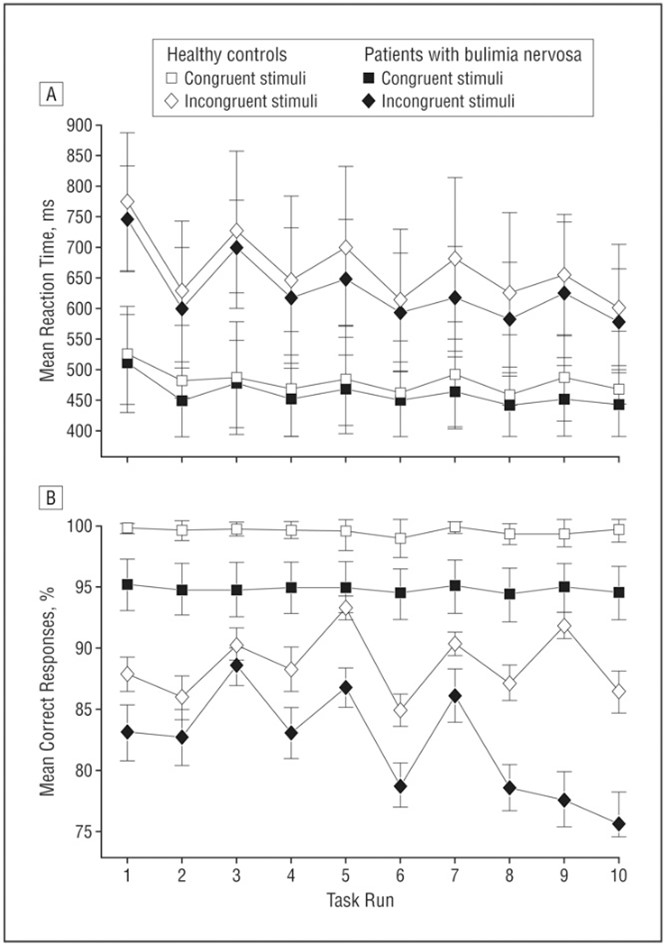
Figure 1- Accuracy and Response time of Bulimia patients and controls.
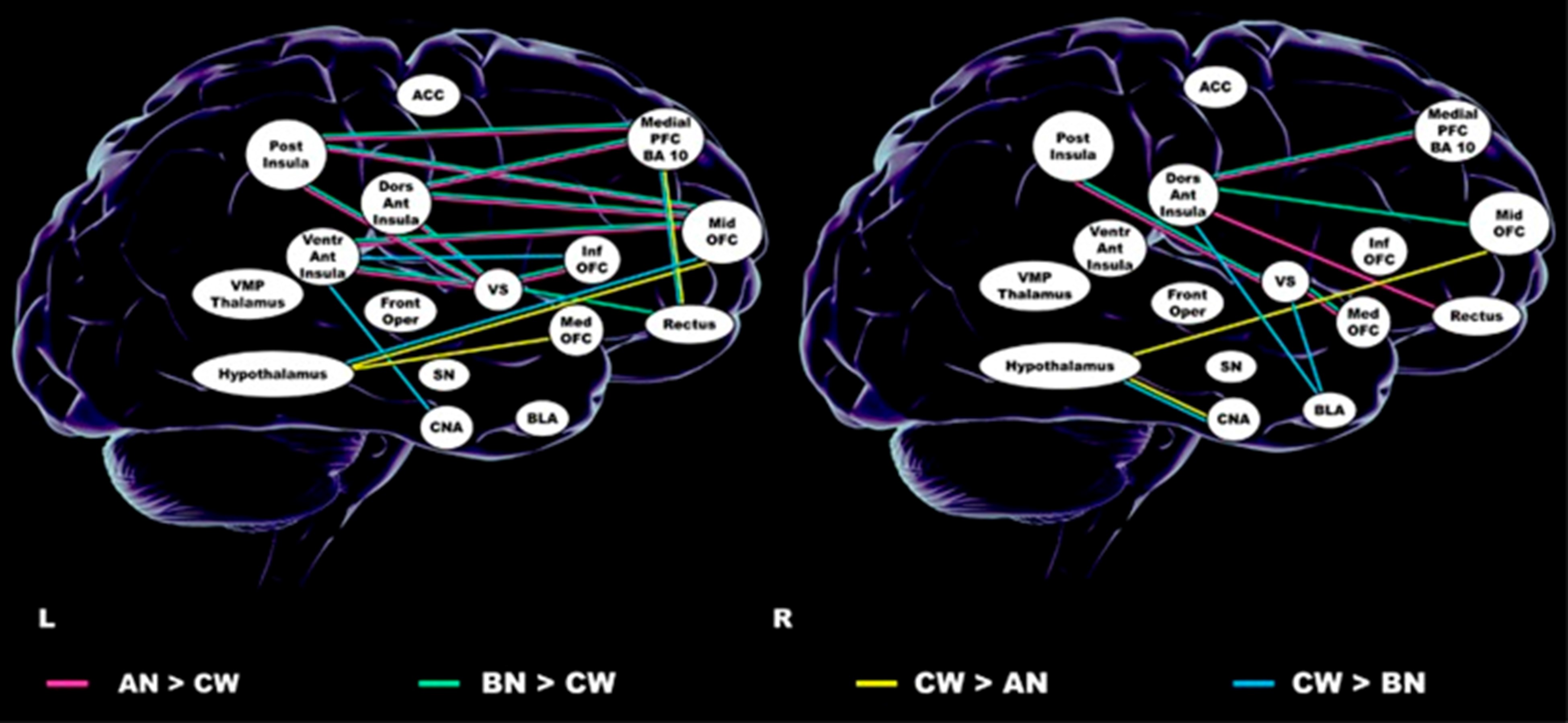
Figure 2- Brain connectivity patterns of AN, BN and healthy participants of study.
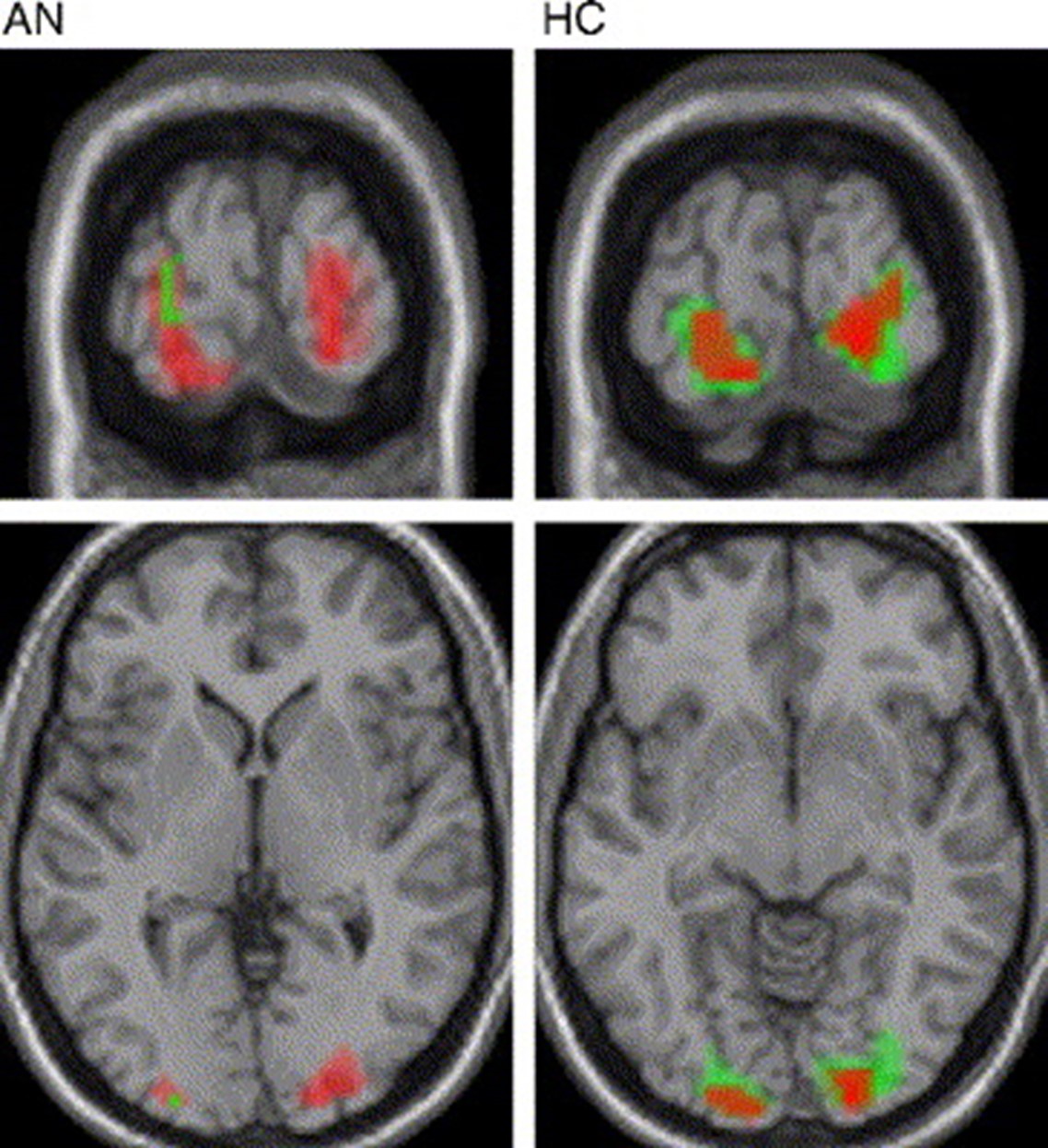
Figure 3- fMRI activation of anorexia nervosa patients and healthy controls.