Diabetes Mellitus
AbdulSamad Olagunju / October 02, 2021
11 min read
Welcome to another awesome blog post! This is a term paper I recently wrote about diabetes mellitus and islet cells.
Quote of the Post:
"Laughter is the best medicine - unless you're diabetic, then insulin comes pretty high on the list." - Jasper Carrott
Introduction
Diabetes is a common chronic illness that affects millions of people worldwide. Around one-tenth of all sufferers of diabetes will have Type 1 Diabetes (T1D), in which an autoimmune response destroys the cells in their pancreas that produce insulin. This disrupts their ability to maintain proper blood sugar levels.
The most common type of treatment for diabetes is the injection of insulin. However, T1D, also called “brittle diabetes,” is especially hard to manage by using insulin injections. One promising research line that may be a viable solution to T1D is islet transplantation. In this procedure, functioning donor pancreas cells are infused into the T1D patient, allowing them to effectively regulate their blood sugar levels. As this paper will illustrate, islet cell transplantation is becoming a practical way to attack the problem of T1D.
Function of β Islet Cells
In the pancreas, β cells are sensitive to the levels of glucose in the blood, efficiently reacting to blood glucose concentrations and releasing insulin when necessary. Insulin signals to cells that they should take up glucose and convert it to stored energy (glucagon). This allows the body to maintain homeostasis, by maintaining optimal glucose levels. In β cells, glucose is taken up by glucose transporters (GLUT2) and metabolized into ATP (2). ATP causes potassium channels on the cell membrane to close, resulting in the depolarization of the cell.
This causes voltage dependent calcium channels to open. An influx of calcium ions causes insulin to be secreted by granules present in the β cell (2). Insulin is released rapidly from granules close to the β cell membrane, and then it is released more gradually from granules that wander to the cell membrane in response to the influx of calcium ions. Insulin travels through capillaries and enters the bloodstream, causing the blood glucose level to decrease via an increase in glycogen synthesis, a reduction in glycogen breakdown, and an increase in the facilitated diffusion of glucose into the muscle and fat cells of the body (13). The release of insulin by β cells is essential for metabolizing glucose in the blood.
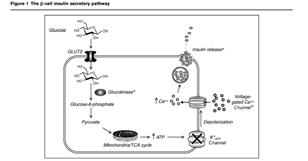
How Glucose triggers the release of Insulin in β cells
Pathophysiology of Type 1 Diabetes Mellitus
In Type 1 Diabetes, immune cells mediate the apoptosis of β cells. Environmental factors play a role in the disease. The mechanisms of these environmental factors are not fully understood due to their complexity, but some of the major factors include obesity, a reduction in the gut microbiota, viral infections, and the foods first introduced to a T1D patient during their childhood (11). The effects of these factors interweave and can create a situation in which an autoimmune response may be activated. Additionally, genetic factors play a role. The most important gene seems to be the one that encodes the human leukocyte antigen (HLA). The HLA is the human MHC complex (6). The MHC complex is very important for presenting antigens to immune cells, and determining which cells are destroyed by the immune system. Variations in this gene may damage the immune self-tolerance mechanism.
Also, individuals who are at high risk to T1D often have developed autoantibodies to important hormones released by the β islet cells such as insulin, and other important molecules to the pancreas such as glutamic acid decarboxylase (11). The presence of multiple autoantibodies to certain compounds often circulate in the blood before the onset of the disease, however researchers believe these autoantibodies do not play a large role in destroying β cells (3). T1D can develop in a myriad of ways, as it is due to a variable combination of environmental and genetic factors that affect immune system (11).
It has been difficult for scientists to surmise the exact molecular basis of the disease due to the difficulties of imaging the pancreas (6). However, it is evident that dendritic cells, T lymphocytes, and B lymphocytes play a significant role in the disease (4). Dendritic cells may engulf β cells due to some triggering event.
In T1D, it is unknown what specifically triggers this process (3). If dendritic cells perform phagocytosis on β cells and present them to CD4+ T cells in the lymph nodes, and these T cells are autoreactive, the immune system will be fully activated. Typically, T cells produced in the thymus must undergo negative selection, a process in which autoreactive cells are destroyed if they do not display self-tolerance.
However, genetic or environmental factors may result in the failure of negative selection in the Thymus, and autoreactive T cells may escape to the rest of the body (3). These T lymphocytes will activate B lymphocytes, causing them to transform into plasma cells and produce autoantibodies to the β cells. These B and T cells will then move to the islets in the pancreas. CD8+ T cells also migrate to the islets to participate in the autoimmune response (6). This coordinated destruction of β cells destroys the body’s ability to manage its blood glucose levels.

Interaction of Immune cells and Beta Cell
In addition, islet cells may be stressed due to an overproduction of insulin due to some infection or inflammatory process (3). The infection may be due to bacteria or viruses, and the inflammatory process may be due to a profusion of cytokines such as IL-10 and IF- γ (6). This may result in sensitization of β cells to the immune system and β cell death (6). Prolonged destruction of β islet cells without treatment results in many long-term complications, which can lead to a comatose state or death. Hyperglycemia, a high level of sugar in the blood, can result in higher risk of cardiovascular disease (11). Furthermore, hyperglycemia can lead to damage to capillaries, causing damage to neurons, the retina, and the kidneys (11).
Islet Transplantation
Nevertheless, these problems may be resolved through islet cell transplantation. The patients usually selected for islet transplantation have experienced severe hypoglycaemic episodes and have unstable Type 1 Diabetes. Insulin injections often have the result of leaving these patients with blood sugar levels that are too low (12). These patients cannot be stabilized with glucose monitoring therapies and insulin pumps (12). Thus, islet transplantation is a way for their body to effectively maintain ideal glucose levels.
In further detail, the process of islet transplantation begins with the procurement of a pancreas from a donor. However, there is limited pancreas availability from deceased donors. This is a potential problem doctors will have to resolve as this treatment becomes more effective and popular. Moreover, islets must be isolated from the pancreas, during which the pancreas is perfused with a cold enzyme solution, then digested (1). The islets are then purified and cultured. These islets are placed in a bag and infused into the liver by a catheter placed into the patient after a small incision on their stomach (1). However, these islets must quickly form connections to new blood vessels, otherwise they will not have enough oxygen to survive. This lack of oxygen coupled with instant blood-mediated inflammatory reaction (complement system and platelets attack islets) destroys up to 60% of new islets in the 2 weeks following the surgery (8). To protect new islets, immunosuppressors are essential (1). Anti-rejection immunotherapies are required for the duration of the patient’s life. This is a major drawback, and a reason why this procedure is not performed on children with Type 1 Diabetes (13). Furthermore, the drugs used as immunosuppressants can limit the ability of the new β cells to release insulin when blood glucose concentrations are high.
Researchers are working to ameliorate the effects of this predicament. A study by Razavi et al. (8), revealed ultrasound therapy aids islet function and revascularization in mice. Figures 3 and 4 in the appendix clearly show how the use of ultrasounds allowed the islets to secrete more insulin and be more vascularized after the transplantation in mice. This implementation of this kind of research in humans has great potential to reduce the number of times patients require islet transplantation and make the procedure more effective. Other risks from the procedure are bleeding in the portal vein (where catheter inserted) and modest pain at the site where the catheter is inserted (12). Altogether, this surgery is regarded as very safe transplantation. Islet transplantation has developed into a standard way to treat T1D.
Conclusion
T1D is an autoimmune disease that obliterates the β cell population in the pancreas, and results in many physiological problems. Thankfully, new methods are making the disease less incapacitating to the lives of the people it affects. Islet cell transplantation remains a promising avenue to fighting this disease. Researchers are continuing to enhance the procedure by improving the access of islets to new blood vessels, ensuring they can survive the transplantation. In the future, it is reasonable to expect that immunosuppressants will have less side effects and will be safer for patients. All in all, islet transplantation may very well become a very dependable and effective way to fight T1D in the future.
References
- Anazawa T, Okajima H, Masui T, and Uemoto S. Current state and future evolution of pancreatic islet transplantation. AGSurg 3(1), 34-42, 2019.
- Fryirs M, Barter PJ, and Rye KA. Cholesterol metabolism and pancreatic beta-cell function. Curr Opin Lipidol. 20(3), 159-64, 2009.
- Ilonen J, Lempainen J, and Veijola R. The heterogeneous pathogenesis of type 1 diabetes mellitus. Nat Rev Endocrinol 15, 635–650, 2019.
- Katsarou A, Gudbjörnsdottir S, Rawshani A, Dabelea D, Bonifacio E, Anderson B, Jacobsen L, Schatz D, and Lernmark A. Type 1 diabetes mellitus. Nat Rev Dis Primers 3, 17016, 2017.
- Kogawa R, Nakamura K, and Mochizuki Y. A New Islet Transplantation Method Combining Mesenchymal Stem Cells with Recombinant Peptide Pieces, Microencapsulated Islets, and Mesh Bags. Biomedicines 8, 299, 2020.
- Morgan N, Leete P, Foulis A, Richardson S. Islet inflammation in human type 1 diabetes mellitus. Life 66(11), 723-734, 2014.
- Nalbach L, Roma L, Schmitt B, Becker V, Körbel C, Wrublewsky S, Pack M, Später T, Metzger W, Menger M, Frueh F, Götz C, Lin H, EM Fox J, MacDonald P, Menger M, Laschke M, and Ampofo E. Improvement of islet transplantation by the fusion of islet cells with functional blood vessels. EMBO Molecular Medicine, 2020.
- Razavi M, Zheng F, Telichko A, Wang J, Ren G, Dahl J, and Thakor AS. Improving the Function and Engraftment of Transplanted Pancreatic Islets Using Pulsed Focused Ultrasound Therapy. Sci Rep 9, 13416, 2019.
- Rickels RM, Robertson RP. Pancreatic Islet Transplantation in Humans: Recent Progress and Future Directions. Endocrine Reviews 40(2), 631–668, 2019.
- Rother KI, Harlan DM. Challenges facing islet transplantation for the treatment of type 1 diabetes mellitus. J Clin Invest. 114(7), 877-883, 2004.
- Saberzadeh-Ardestani B, Karamzadeh R, Basiri M, Hajizadeh-Saffar E, Farhadi A, Shapiro AMJ, Tahamtani Y, and Baharvand H. Type 1 Diabetes Mellitus: Cellular and Molecular Pathophysiology at A Glance. Cell J. 20(3), 294-301, 2018.
- Shapiro A, Pokrywczynska M, and Ricordi C. Clinical pancreatic islet transplantation. Nat Rev Endocrinol 13, 268–277, 2017.
- Wilcox G. Insulin and insulin resistance. Clin Biochem Rev. 26(2), 19-39, 2005.
Appendix
The process in which Glucose causes β cells to release Insulin. From reference 2.
The cells with a significant response in the immune system’s destruction of β cells. From Reference 4.

A graph showing the microvessels density when islets are treated with ultrasound therapy (islets and pFUS), and when they are not treated at all after they have been infused into a mouse with T1D. The islets treated with ultrasound therapy had a significantly higher amount of vascularization that the control islets. Research from Reference 8.

The islets that received a high dose of ultrasound had the highest secretion of insulin by a significant amount. They also had a higher insulin content by a significant amount. This experiment was performed on a mouse. Research from Reference 8.
On to the next, thanks for reading.
