ADHD and NEIM
AbdulSamad Olagunju / May 05, 2023
32 min read
Welcome to another awesome blog post! This is a term paper I recently wrote about ADHD.
Quote of the Post:
"Given their automatic tuning out, ADD children forever find themselves being told to “pay attention”—a demand that completely misunderstands both the nature of the child and the nature of attention. The obvious monetary connotation of “pay” is that attention is something the child owes the adult, that the child’s attention belongs to the adult by right. The phrase takes for granted that being attentive is always a consciously chosen act, subject to one’s will. Both of these assumptions are faulty." - Gabor Maté
Introduction
A Case Study on the Failures of Current ADHD Treatments
A 12-year-old girl was brought to her doctor with her mother complaining of poor academic performance and concentration in class (1). As cases of attention deficit/hyperactivity disorder (ADHD) were identified in her family tree, she was prescribed with a drug called Adderall. For the following month, the girl reported to her doctor that she no longer had problems with inattention. Her mother proudly reported that her grades were significantly higher. Things were looking much better. Unfortunately, one week later this girl suffered from an anxiety attack. She struggled with visual hallucinations, psychomotor retardation, and maintaining proper hygiene. This girl had gone through amphetamine-induced psychosis due to her usage of Adderall (1). Her ADHD diagnosis resulted in prescription of a drug that left her incoherent and unstable.
ADHD is a disease of impulsivity. The prevalence of ADHD worldwide ranges from 2.2 to 17.8% (2). ADHD patients have a host of other comorbidities, such as higher risk of vehicular accidents due to increased impulsivity levels. Currently, pharmaceutical drugs used to treat ADHD fail to serve as a long-term solution, despite their short-term efficacy (3). In addition, 30% of ADHD patients cannot tolerate the side effects of their ADHD drugs. Current drug treatments for ADHD have an abundance of risk factors and fail to change detrimental long-term outcomes for ADHD patients (4). The chilling experience undergone by this girl illustrates this point. It is of the utmost importance that ADHD patients understand how best to manage their symptoms given the myriad of risks associated with ADHD. Most ADHD drugs target the central nervous system; however, dysregulation of the endocrine and immune system also affect ADHD phenotypic behaviours. Ironically, physicians have been unable to control their own impulses in prescribing powerful drugs like Adderall in order to treat ADHD. This needs to change. By harnessing the power of neural, endocrine, and immunomodulatory interactions, researchers can give ADHD patients better and more effective ways to manage their symptoms.
SECTION 1: A Traditional Understanding of ADHD
1.1 – What is ADHD?
ADHD has a diverse range of manifestations (5). It is considered a disorder of neurodevelopment. ADHD patients suffer from impulsive behaviour, hyperactivity, and struggle with excess levels of inattention. Symptoms are often diagnosed at a young age in patients. Patients with ADHD may struggle achieving high marks in school and performing well in their careers. ADHD patients may also struggle in social situations due to their predisposition towards impulsive behaviour.
A population-based survey showed that most male ADHD patients were diagnosed at 12, whereas females were diagnosed most frequently at the age of 16 (6). 64% of ADHD patients also had another condition, most commonly anxiety disorders. 62% of children in the U.S. with ADHD in 2016 were taking medication. 23 billion dollars are spent in the U.S. every year on treating ADHD, and it is estimated that between 38 and 72 billion dollars are lost due to ADHD associated reduced productivity. ADHD is a disease with clear social and economical ramifications for individuals and society.
1.2 – Etiology and Pathophysiology of ADHD
The etiology of ADHD is complex. Research has indicated ADHD is hereditary (1, 2). Different genes play important roles in ADHD pathology. These include genes encoding cell migration, neural development, and dopamine transporters/receptors (5, 7). There are several environmental factors associated with higher risk of ADHD. They include heavy metal exposure and pesticide exposure. Moreover, environmental factors such as nutritional deficiencies, maternal alcohol consumption, and exposure to viral infections play a role in ADHD pathology (5, 22).
Regardless of this previous research, the causes of ADHD are still not fully understood. Several mechanisms have been proposed. Many ADHD studies focus on the role of dopaminergic, noradrenergic, and serotonergic signaling (7). In addition, structural changes in the brain have been associated with ADHD (8). Traditional research into ADHD focuses on the role of neurotransmitters in the brain, brain volume differences, and genetic studies (5). Unfortunately, as ADHD is a clinical diagnosis, there is a lack of standardization in ADHD research. This can make it difficult to answer mechanistic questions concerning ADHD disease pathology.
Research into the brain has still uncovered patterns concerning ADHD pathophysiology. An MRI neuroimaging study, a mega-analysis, revealed subcortical brain volume differences among ADHD patients (8). There were 1713 ADHD patients and 1529 controls. Researchers observed significantly smaller volumes in the nucleus accumbens, amygdala, caudate nucleus, hippocampus, and putamen when comparing ADHD patients to controls. The largest difference was found in the amygdala. Problems with the amygdala are associated with the emotional difficulties that ADHD patients face, such as reduced emotional reactions to stimuli that provide satisfaction. These results have pushed forward the interpretation of ADHD as primarily a disorder of the brain. ADHD was also associated with a 3% decrease in global brain volume (9). Moreover, there was no association with stimulant medication and changes in brain volume among ADHD patients (8). Treatments for ADHD are failing to result in global brain changes and long-term solutions for ADHD patients (8). Nonetheless, the focus in ADHD research has been on the role of the central nervous system, and the immune and endocrine system have been neglected.
1.3 - Current Treatment Strategies for ADHD
The major form of treatment for ADHD patients involves stimulant and non-stimulant pharmaceuticals (5). Behavioural treatments are also common. As dopaminergic signaling plays a large role in ADHD, medications affect dopamine release or reuptake. Most ADHD drugs increase the availability of dopamine. Unfortunately, ADHD drugs have a myriad of side effects, including a decrease in appetite, changes in blood pressure, and an increased risk of drug dependency. Psychosocial and behavioural treatments are available, but research indicates that medication currently provides more efficacious outcomes. ADHD research currently focuses on the neural aspects of the disease but overlook the importance of neuro-endocrine and neuroimmune interactions. Moreover, the random control trials used to establish the safety and efficacy of ADHD drugs fail to account for patients with higher severity of ADHD symptoms (10). This leads to worse clinical outcomes for these patients using ADHD drugs. In addition, there is a lack of evidence supporting the safety of long-term use of ADHD medications. ADHD patients have misconceptions about the safety of their medications. For example, ADHD stimulant medication has a significant association with psychotic disorders. Moreover, ADHD medications require prescriptions, and compliance from ADHD patients is poor (around 64%) (11). Another study found that the attitudes common among parents of patients with ADHD include the belief that ADHD medications have adverse side effects (12). The public has a clear distrust of the safety of ADHD drugs.
A research survey indicated that 71% of ADHD patients suffer from side effects, ranging from sleep problems to loss of appetite. Common medications for ADHD include stimulants such as amphetamine and methylphenidate (13, 14). When high dosages of methylphenidate were administered to young male rats, this led to increases in mitochondrial superoxide production in the cerebellum (14). Superoxide is a reactive oxygen species. It leads to further increases in the production of central nervous system proinflammatory cytokines. The activation of immune cells and increases in inflammation may play a role in ADHD-related side effects. More research still needs to be performed to answer the mechanistic questions concerning methylphenidate and its side effects on the body.
Cognitive behavioral therapy is often also used to treat ADHD. Cognitive behavioural therapy for adult Chinese ADHD patients resulted in significant improvements in impulsivity levels (15). In addition, a meta-analysis revealed that cognitive behavioral therapy results in significant improvements of ADHD symptoms (16). Cognitive behavioural therapy provides an alternative method for treating ADHD. Other therapies may be viable and effective, but further research involving immune and endocrine associated ADHD mechanisms in these therapies are currently lacking. Using medication to treat ADHD relies on interactions between psychiatrists, pharmacists, and several other health care practitioners to treat the disease (5). This, along with the costs of medication, make treating ADHD expensive and time-consuming. Moreover, patient noncompliance with medications is commonplace, and the public is beginning to mistrust ADHD drugs due to dangerous side-effects. This over-reliance on treating ADHD with drugs must come to an end. A new paradigm involving neuro-endo-immunomodulation (NEIM) for treating ADHD is required to rebuild trust with the public, provide better long-term outcomes for ADHD patients, and reduce costs for the health-care system (5).
SECTION 2: A NEIM Approach to ADHD
2.1 – Preliminary Evidence for NEIM Interactions in ADHD
Research indicates that the neural, immune, and endocrine systems all play a role in ADHD. Researchers used spontaneously hypertensive rats (SHR), a rodent ADHD model, to study immune and endocrine influences in ADHD development (7). Due to the predisposition of males to ADHD, male rats were used in this study. To determine cytokine expression, ELISA experiments were performed. In addition, immunohistochemical methods were performed in order to learn about neurochemical alterations. Juvenile ADHD model rats had significantly higher levels of pro-inflammatory markers such as interleukin 1-beta (Figure 1) in addition to oxidative stress markers. Mature ADHD model rats had elevated serum and adrenal levels of hormones such as cortisol. ADHD rats had lower medial prefrontal cortex volumes in addition to higher expression of dopamine receptors. This study shows that it is possible to study ADHD from a NEIM perspective. In animal models, the immune and endocrine system may play a role in ADHD pathogenesis, in addition to neural circuitry. For the rest of this review, further research indicating the interactions between the neural, endocrine, and immune system will be highlighted.
2.2 – Stress and the HPA Axis in ADHD
ADHD involves the activity of several physiological systems. This includes the endocrine and immune system. The endocrine system involves the secretion of hormones, and the hypothalamic pituitary axis plays a large role in this process. The Hypothalamic Pituitary Axis (HPA) is extremely important for the regulation of homeostasis. The hypothalamus secretes corticotropin releasing hormone, which stimulates adrenocorticotropin hormone release from the pituitary, which in turn stimulates the secretion of cortisol from the adrenal cortex. Stress activates the adrenocortical response, leading to the secretion of glucocorticoids by the adrenal cortex.
In a longitudinal study focusing on Dutch adolescents from the ages of 11 to 19, DSM based ADHD, anxiety, and depression values were collected (17). In addition, other questionnaires collected data based on stress exposure. Trajectories were then modeled. Results showed stress exposure levels were higher in the ADHD subgroups. ADHD patients that were exposed to lower levels of stress over time also had higher remission rates of ADHD. However, this study only shows correlations and fails to take into account the mechanisms that result in an association of higher stress levels and ADHD. Nevertheless, it shows that chronically high stress levels may play a role in the persistence of ADHD.
High levels of stress exposure affect the body’s ability to secrete glucocorticoids. A study found that ADHD Chinese male children had significantly lower plasma cortisol levels when compared to controls (18). This suggests that HPA axis dysfunction plays a role in ADHD. If patients have an impaired ability to secrete glucocorticoids, they will struggle with dealing with stressful situations. This lack of cortisol in addition to increased stress exposure levels may lead to a vicious cycle of stress in ADHD patients, leading to the development or exacerbation of ADHD symptoms. Glucocorticoids also play a role in learning, memory, and attention, which are affected in subjects with ADHD. Cortisol also plays an important role in the body by limiting the severity of the stress response. A lack of cortisol may contribute to a reduced ability of cortisol to prevent increased stress levels from compromising homeostatic processes.
Another cohort of patients with ADHD also had lower salivary cortisol levels when compared to age and sex matched controls (19). In addition, injecting high levels of cortisol in pregnant rats resulted in offspring displaying behavioural characteristics similar to those of ADHD animal models (20). This reveals that dysfunction of the HPA axis may play a role in the development of ADHD. More research into hormones and endocrine signaling in ADHD may reveal why ADHD patients exhibit these physiological differences. This research provides a rationale for the importance of treating the HPA axis and limiting stress in patients with ADHD.
2.3 – The Immune System in ADHD
There are studies linking the role of the endocrine system in ADHD pathogenesis, however, what role does the immune system play? It is evident that there is a great deal of interactions between the immune and endocrine system. When exposed to pathogens, the immune system is activated. Immune cells produce cytokines and other mediators of inflammation. These molecules also act at the pituitary and hypothalamus to trigger release of adrenocorticotropic hormone and corticotropin releasing hormone, respectively. These molecules trigger the release of glucocorticoids by the adrenal cortex. Glucocorticoids act to reduce the severity of the immune response. To maintain homeostasis, glucocorticoids play an important role in the immune and stress response. The presence of glucocorticoids acts as a buffer, preventing the overactivity or over suppression of the immune response. As previous evidence indicates the glucocorticoid production is disrupted among patients with ADHD, this may also lead to disruptions in the immune system. Indeed, research indicates that an overactive immune system may play a role in ADHD pathogenesis.
Behavioural and psychiatric disorders such as ADHD can often occur as a result of autoimmune disease. Autoimmune disorders occur due to inappropriate activation of the inflammatory system. An overactivation of the inflammatory system can result in damage to an organism’s cells by the very mechanisms meant to preserve homeostasis. Autoimmunity can result in damage to endocrine glands and neuronal structures. Many autoimmune disorders are associated with ADHD (21). Patients with autoimmune disorders such as arthritis juvenilis and autoimmune thyroiditis have a higher risk of ADHD. Maternal autoimmune diseases are also associated with ADHD. In children with a family history of autoimmune disorders such as type 1 diabetes and psoriasis, they have an increased risk of ADHD. Type 1 diabetes (T1D) is due to the T cell mediated destruction of beta islet cells of the pancreas. It is an example of how increased pro-inflammatory activity may be involved in ADHD pathogenesis. Moreover, another prospective nation-wide (Norway) study showed that mothers with ADHD offspring had higher rates of autoimmune diseases such as multiple sclerosis, type 1 diabetes, and rheumatoid arthritis (22). Other autoimmune disorders with a profound inflammatory component such as type 2 diabetes showed no association with ADHD. More research is required in order to learn more about the specific autoimmune mechanisms involved in disorders such as T1D that may increase ADHD risk. These results provide a clear association between autoimmune disorders and ADHD, implicating the immune system in ADHD pathogenesis.
Additionally, ADHD children have significantly increased levels of auto-antibodies to the Purkinje cells of the cerebellum (23). This study indicates the antibodies may serve as biomarkers for autoimmunity in ADHD. The cerebellum plays a role in attentional learning and the regulation of emotions and is closely involved with the basal ganglia and the prefrontal cortex, other regions implicated in ADHD by volumetric imaging studies (23). Auto-antibodies to the dopamine transporter were higher among ADHD patients (24). Antibodies represent a way for the immune and neural systems to interact. As ADHD is considered a neurobehavioral disease, it is important to understand how the immune system may affect the brains of ADHD patients.
Another study also found that children with ADHD have significantly higher serum levels of interleukin-6 (IL-6), a pro-inflammatory cytokine, when compared to controls (25). IL-6 may be involved in the mediation of inflammatory signals in ADHD. When the immune system mounts a response against peripheral endotoxins, IL-6 release is mediated by hypothalamic neurons. IL-6 is also released by microglia, and it is pro-phagocytotic, so it may be a possible mechanism for demyelination and a loss of white matter in ADHD. This evidence shows how neuro-immune communication may be involved in ADHD pathogenesis. Targeting increased inflammation or autoimmune mechanisms may be another viable way to limit the severity of ADHD in patients.
2.4 – Dopaminergic/Noradrenergic Signaling in ADHD
Dopamine also plays a significant role in regulating homeostasis, and dopaminergic signaling is impaired in ADHD (26). Immune cells produce dopamine in order to communicate with neural circuits. Dopamine is involved with the activation of immune cells, and as previously discussed, ADHD is associated with autoimmune disorders. Many studies have shown that ADHD is associated with mutations to the human dopamine transporter (DAT1) gene (27). These mutations result in reduced dopaminergic signaling. A prospective longitudinal study in male adolescents revealed there is a significant association between the DAT1 genotype and exposure to prenatal smoke. Prenatal smoke exposure is an environmental risk factor for ADHD. Moreover, the striatum of males shows greater dopamine receptor density when compared to females, and this may be a reason why males are more vulnerable to ADHD (28). Sexual dimorphisms often indicate the presence of endocrine related signaling, further highlighting the importance of exploring endocrine mechanisms in ADHD pathology.
Researchers used positron emission tomography to measure dopamine transporters and receptors (29). ADHD patients had lower specific binding of neural cells in the dopamine reward pathway in the left side of the brain. The dopamine reward pathway is the meso-accumbens dopamine pathway. The major site activated by rewards is the nucleus accumbens, and the midbrain is also involved in motivation circuity. ADHD patients had less D2/D3 receptors in addition to less dopamine transporter availability. An inattention phenotype may be due to a reduction in synaptic markers for dopamine in patients with ADHD. This study shows that without sufficient dopamine signaling, ADHD patients may struggle with overcoming their attentional deficits without pharmacological support. Moreover, children and adolescents show significant differences in the dopaminergic property of their midbrain nuclei when compared to controls (30). It is likely that impaired dopaminergic signaling in the brain plays a significant role in ADHD. In addition, animal models of ADHD involving spontaneously hypertensive rats indicate downregulation of dopamine receptors in the brain contributes to ADHD (31). Increasing the availability of dopamine is the primary way that medications treat ADHD. Nevertheless, there are other mechanisms that may play a role in ADHD pathology, and the heavy involvement of dopamine in the immune system indicate that by intervening in these mechanisms, new therapeutic benefits may be available for patients with ADHD.
Dopamine is not the only neurotransmitter that plays a role in ADHD (32). Reductions in norepinephrine signaling are associated with ADHD. The locus coeruleus is the major source of norepinephrine in the brain. The locus coeruleus is involved in regulating working memory and sending norepinephrine projections to the prefrontal cortex. The prefrontal cortex is responsible for executive functions, many of which are impaired in patients with ADHD (32). Moreover, stress results in the activation of the locus coeruleus. Norepinephrine plays a significant role in the activation of the stress system. Norepinephrine transmission is reduced in patients with ADHD (32). Normally, norepinephrine decreases the activity of the prefrontal cortex in response to sensory stimuli. This has been hypothesized to result in better focus and attention levels. Atomoxetine has been used to treat ADHD (33). Atomoxetine is a norepinephrine transporter inhibitor. Norepinephrine transporters increase the clearance of norepinephrine released at the synapse. Blocking norepinephrine transporters increases the neurotransmission of norepinephrine. In rats, atomoxetine blocks depletion of norepinephrine (32). Norepinephrine concentrations in the prefrontal cortex were increased by atomoxetine. These increases in norepinephrine signaling improve the stress response and attentional awareness. Dopamine and noradrenergic signaling both play an important role in ADHD pathophysiology and thus are the target for most pharmaceutical drugs for ADHD.
2.5 – The Gut Microbiome in ADHD:
Gut bacteria modulate neurotransmitter levels. Therefore, they may also play a role in ADHD pathology. Researchers have collected fecal samples from patients with ADHD and controls and found significant differences in some bacteria (34). The Ruminococcaceae genus was abundant in patients with ADHD. Other research has shown the Ruminococcaceae genus is prevalent in individuals with autism, anxiety, and bipolar disorder. These bacteria degrade cellulose, converting it to short chain fatty acids. These chemicals cause free fatty acid receptors to be activated and allow microglia to develop into a neuroprotective phenotype. Short chain fatty acids can act systemically or locally and modulate neuronal functioning via autonomic and sensory innervation in the gut. Pathogenic gut bacteria can also increase systemic inflammation in the body, contribute to leaky gut syndrome, and alter the phenotype of microglia to become more toxic. When ADHD gut bacteria are introduced to mice, anxiety behaviors are more likely to be observed (34). Early studies show the gut microbiome plays a role in ADHD. However, the exact mechanisms in which these bacteria affect the neural, endocrine, and immune systems remains unknown.
Gut bacteria are involved in the production of precursors for important neurotransmitters like serotonin and dopamine (35). Researchers characterized the gut bacteria of ADHD patients using 16S rRNA gene sequencing, learning that ADHD patients had significantly higher numbers of Bifidobacterium when compared to controls. Researchers also discovered higher levels of an enzyme called cyclohexadienyl dehydratase in ADHD patients. Cyclohexadienyl dehydratase is involved in the generation of phenylalanine, a precursor of dopamine. Bifidobacterium levels were associated with the increases in the levels of this enzyme. Further research is required to understand the mechanisms in which Bifidobacterium contribute to ADHD pathology. Nevertheless, these studies indicate these specific bacteria in the gut may be involved in the dysregulation of dopaminergic signaling.
In addition, researchers used an SHR ADHD rat model to study inflammation and microglial function (36). A healthy gut microbiome is essential for the proper development of microglia. They found that Iba1 (marker for microglia) expression was higher among ADHD rats when compared to controls. Dysfunction of the gut microbiome may be related to dysregulation of microglia pruning and increased activation of microglia. SHR rats have limitations, including increases in dopamine/norepinephrine as rats age, leading to decreased ADHD symptoms. Further animal models for ADHD are required in order to further validate these results. Nevertheless, researchers measured the brains of human ADHD patients and controls using PET imaging. They found that patients with ADHD had increased numbers of activated microglia in the orbito-frontal and dorsolateral prefrontal cortex when compared with controls. The activation of these microglia was associated with increased inattention among ADHD patients. As short chain fatty acid production from gut bacteria modulates microglial development, the gut microbiome may play a role in the activation of microglia in ADHD. These studies provide evidence that dysfunction of the gut microbiome is involved with ADHD pathogenesis.
2.6 - NEIM Therapies and ADHD:
Finding better ways to treat ADHD patients is crucial. Parents for children with ADHD had significantly higher levels of anxiety, perceived stress, and reported physical health problems at a higher frequency when compared to controls (37). In addition, they had higher levels of C-reactive protein, a marker for inflammation. Finding ways to reduce the severity of ADHD symptoms can benefit both the quality of their lives and their caregiver’s lives.
Yoga results in changes to gene expression that protect cells from injury. Furthermore, evidence suggests that yoga inhibits the chronic activation of glucocorticoid pathways via the HPA axis. Dementia caregivers undergo a lot of stress . Nevertheless, 8 weeks of yogic mediation caused circulating leukocytes to reduce their expression of metastasis and proinflammatory related genes among dementia caregivers. This provides evidence that yoga is involved in physiological pathways that reduce stress. A study found a significant improvement in ADHD symptoms after an average of 8 yoga training sessions were given to children diagnosed with ADHD (38). Other studies have shown that treatment of ADHD using yoga and medications stabilize ADHD symptoms.
Traditional Chinese medicines such as acupuncture and Tai chi were found to be as effective as methylphenidate in ADHD treatment for short durations of time. Unfortunately, the studies were not of a rigorous methodological standard, and more studies are required to fully validate this claim. A Tai Chi study involving undergraduate ADHD students did show that retention rates were high, indicating the patients with ADHD will adhere to this form of treatment (39). In other tai chi studies, teachers reported that ADHD symptoms improved among subjects following a 5-week tai chi course (40). Whether these changes are long-term or result in plasticity induced changes to the brain remains to be answered. Moreover, a study involving ADHD rats (Adult male SHR) showed improvements in spatial learning ability after 30 minutes per day of treadmill exercise (41). Young men with symptoms of ADHD reported reduced feelings of depression, and increased motivation for cognitive tasks following cycling (42). Physical activities such as yoga, tai chi, and exercise are affordable and high compliance, and may be a possible way of alleviating the symptoms of ADHD.
Researchers also placed children diagnosed with ADHD on a specific hypoallergenic diet (43). Foods containing milk, eggs, artificial preservatives, and gluten were excluded in addition to other substances. ADHD symptoms were found to be correlated with carbohydrate intake, and the diet modification program improved ADHD symptoms. Changing a patient’s diet may be a promising therapeutic avenue for patients with ADHD. Dietary supplementation of vitamin D may be another possible means of improving ADHD symptoms. Children with ADHD expressed significantly lower levels of serum vitamin D when compared to controls (44). A deficiency in vitamin D has been found to be associated with a dysfunctional immune system and increased antibody production. The food that individuals consume affect the function of their gut bacteria. More research needs to be performed in order to learn more about the nutritional factors that affect ADHD and how dietary changes may attenuate symptoms of ADHD. More studies are required to address the gaps of knowledge involving controlling inflammation and oxidative stress involved in ADHD, and the dysregulation of the HPA axis. Nevertheless, yoga, tai chi, exercise, and dietary changes may provide alternatives to classic pharmacological treatments for ADHD.
Conclusion: NEIM offers an Alternative Way to Treat ADHD
ADHD is not a one-dimensional disease. It involves the interaction between several different systems in the human body. To better help ADHD patients, researchers must be prepared to broaden their traditional understanding of the pathophysiology of ADHD. The nervous system is key to understanding ADHD pathophysiology, as evidenced by the widespread use of stimulants in treating ADHD. Unfortunately, current drugs are too expensive and have too many adverse side effects. Caregivers and ADHD patients distrust these therapies. Regulating stress, inflammation associated with autoimmunity, and gut microbiomes may provide previously unknown therapeutic benefits for ADHD patients. More animal models and clinical trials with ADHD patients need to be performed that involve other avenues such as mind body therapy and dietary changes. By introducing activities that have less side effects such as yoga and exercise, or are significantly cheaper than drugs, such as dietary changes, ADHD patients will pay less and suffer less for their treatments. The body relies on the systemic harmony of the endocrine, neural, and immune system. ADHD treatments should reflect this paradigm.
References
- Surles LK, May HJ, and Garry JP. Adderall-induced psychosis in an adolescent. The Journal of the American Board of Family Practice 15(6): 498–500, 2002.
- Sharma A, Couture J. A review of the pathophysiology, etiology, and treatment of attention-deficit hyperactivity disorder (ADHD). Annals of Pharmacotherapy 48: 209– 225, 2013.
- Szopinska-Tokov J, Dam S, Naaijen J, Konstanti P, Rommelse N, Belzer C, Buitelaar J, Franke B, Aarts E, Arias Vasquez A. Investigating the gut microbiota composition of individuals with attention-deficit/hyperactivity disorder and association with symptoms. Microorganisms, 2020.
- Núñez-Jaramillo L, Herrera-Solís A, Herrera-Morales WV. ADHD: Reviewing the causes and evaluating solutions. Journal of Personalized Medicine 11: 166, 2021.
- Magnus W, Nazir S, Anilkumar AC, and Shaban K. Attention Deficit Hyperactivity Disorder, 2022.
- Danielson ML, Bitsko RH, Ghandour RM, Holbrook JR, Kogan MD, Blumberg SJ. Prevalence of parent-reported ADHD diagnosis and associated treatment among U.S. children and adolescents, 2016. Journal of Clinical Child & Adolescent Psychology 47: 199–212, 2018.
- Kozłowska A, Wojtacha P, Równiak M, Kolenkiewicz M, Huang AC. ADHD pathogenesis in the immune, endocrine and nervous systems of juvenile and maturating SHR and Wky Rats. Psychopharmacology 236: 2937–2958, 2019.
- Hoogman M, Bralten J, Hibar DP, Mennes M, Zwiers MP, Schweren LS, van Hulzen KJ, Medland SE, Shumskaya E, Jahanshad N, Zeeuw Pde, Szekely E, Sudre G, Wolfers T, Onnink AM, Dammers JT, Mostert JC, Vives-Gilabert Y, Kohls G, Oberwelland E, Seitz J, Schulte-Rüther M, Ambrosino S, Doyle AE, Høvik MF, Dramsdahl M, Tamm L, van Erp TG, Dale A, Schork A, Conzelmann A, Zierhut K, Baur R, McCarthy H, Yoncheva YN, Cubillo A, Chantiluke K, Mehta MA, Paloyelis Y, Hohmann S, Baumeister S, Bramati I, Mattos P, Tovar-Moll F, Douglas P, Banaschewski T, Brandeis D, Kuntsi J, Asherson P, Rubia K, Kelly C, Martino AD, Milham MP, Castellanos FX, Frodl T, Zentis M, Lesch K-P, Reif A, Pauli P, Jernigan TL, Haavik J, Plessen KJ, Lundervold AJ, Hugdahl K, Seidman LJ, Biederman J, Rommelse N, Heslenfeld DJ, Hartman CA, Hoekstra PJ, Oosterlaan J, Polier Gvon, Konrad K, Vilarroya O, Ramos-Quiroga JA, Soliva JC, Durston S, Buitelaar JK, Faraone SV, Shaw P, Thompson PM, Franke B. Subcortical brain volume differences in participants with attention deficit hyperactivity disorder in children and adults: A crosssectional mega-analysis. The Lancet Psychiatry 4: 310–319, 2017.
- Castellanos FX. Developmental trajectories of brain volume abnormalities in children and adolescents with attention-deficit/hyperactivity disorder. JAMA 288: 1740, 2002.
- Chang Z, Ghirardi L, Quinn PD, Asherson P, D’Onofrio BM, Larsson H. Risks and benefits of attention-deficit/hyperactivity disorder medication on behavioral and neuropsychiatric outcomes: A qualitative review of pharmacoepidemiology studies using linked prescription databases. Biological Psychiatry 86: 335–343, 2019.
- Kamimura-Nishimura KI, Brinkman WB, and Froehlich TE. Strategies for improving ADHD medication adherence. Current psychiatry, 18(8), 25–38, 2019.
- Toomey SL, Sox CM, Rusinak D, Finkelstein JA. Why do children with ADHD discontinue their medication? Clinical Pediatrics 51: 763–769, 2012.
- Sahin S, Yuce M, Alacam H, Karabekiroglu K, Say GN, Salıs O. Effect of methylphenidate treatment on appetite and levels of leptin, ghrelin, adiponectin, and brain-derived neurotrophic factor in children and adolescents with attention deficit and hyperactivity disorder. International Journal of Psychiatry in Clinical Practice 18: 280– 287, 2014.
- Gomes KM, Inácio CG, Valvassori SS, Réus GZ, Boeck CR, Dal-Pizzol F, Quevedo J. Superoxide production after acute and chronic treatment with methylphenidate in young and adult rats. Neuroscience Letters 465: 95–98, 2009.
- Huang F, Tang Y-lang, Zhao M, Wang Y, Pan M, Wang Y, Qian Q. Cognitivebehavioral therapy for adult ADHD: A randomized clinical trial in China. Journal of Attention Disorders 23: 1035–1046, 2017.
- Auclair V., Harvey PO, and Lepage M. La thérapie cognitive-comportementale dans le traitement du TDAH chez l'adulte [Cognitive Behavioral Therapy and the Treatment of ADHD in Adults]. Sante mentale au Quebec, 41(1), 291–311, 2016.
- Hartman CA, Rommelse N, van der Klugt CL, Wanders RBK, Timmerman ME. Stress exposure and the course of ADHD from childhood to young adulthood: Comorbid severe emotion dysregulation or mood and anxiety problems. Journal of Clinical Medicine 8: 1824, 2019.
- Ma L, Chen Y-H, Chen H, Liu Y-Y, Wang Y-X. The function of hypothalamus–pituitary– adrenal axis in children with ADHD. Brain Research 1368: 159–162, 2011.
- El Ghamry RH, Mohamed MM, Azzam HM, Elhabiby MM, Hasan HM, Hashish AF, Elhamshary MM, Barakat DM. Aggression in ADHD: Relation to salivary cortisol. Middle East Current Psychiatry 28, 2021.
- Jeon S-C, Kim H-J, Ko E-A, Jung S-C. Prenatal exposure to high cortisol induces ADHD-like behaviors with delay in spatial cognitive functions during the post-weaning period in rats. Experimental Neurobiology 30: 87–100, 2021.
- Nielsen PR, Benros ME, Dalsgaard S. Associations between autoimmune diseases and attention-deficit/hyperactivity disorder: A nationwide study. Journal of the American Academy of Child & Adolescent Psychiatry 56, 2017.
- Instanes JT, Halmøy A, Engeland A, Haavik J, Furu K, Klungsøyr K. Attentiondeficit/hyperactivity disorder in offspring of mothers with inflammatory and immune system diseases. Biological Psychiatry 81: 452–459, 2017.
- Passarelli F, Donfrancesco R, Nativio P, Pascale E, Trani MD, Patti AM, Vulcano A, Gozzo P, Villa MP. Anti-purkinje cell antibody as a biological marker in attention deficit/hyperactivity disorder: A pilot study. Journal of Neuroimmunology 258: 67–70,
- Giana G, Romano E, Porfirio MC, D'Ambrosio R, Giovinazzo S, Troianiello M, Barlocci E, Travaglini D, Granstrem O, Pascale E, Tarani L, Curatolo P, Laviola G, Adriani W. Detection of auto-antibodies to DAT in the serum: Interactions with DAT genotype and psycho-stimulant therapy for ADHD. Journal of Neuroimmunology 278: 212–222, 2015.
- Darwish AH, Elgohary TM, Nosair NA. Serum interleukin-6 level in children with attention-deficit hyperactivity disorder (ADHD). Journal of Child Neurology 34: 61–67,
- del Campo N, Chamberlain SR, Sahakian BJ, Robbins TW. The roles of dopamine and noradrenaline in the pathophysiology and treatment of attention-deficit/hyperactivity disorder. Biological Psychiatry 69, 2011.
- Becker K, El-Faddagh M, Schmidt MH, Esser G, Laucht M. Interaction of dopamine transporter genotype with prenatal smoke exposure on ADHD symptoms. The Journal of Pediatrics 152, 2008.
- Andersen SL, Teicher MH. Sex differences in dopamine receptors and their relevance to ADHD. Neuroscience & Biobehavioral Reviews 24: 137–141, 2000.
- Volkow ND, Wang G-J, Kollins SH, Wigal TL, Newcorn JH, Telang F, Fowler JS, Zhu W, Logan J, Ma Y, Pradhan K, Wong C, Swanson JM. Evaluating dopamine reward pathway in ADHD. JAMA 302: 1084, 2009.
- Ernst M, Zametkin AJ, Matochik JA, Pascualvaca D, Jons PH, Cohen RM. High midbrain [18f]dopa accumulation in children with attention deficit hyperactivity disorder. American Journal of Psychiatry 156: 1209–1215, 1999.
- Satoh H, Suzuki H, Saitow F. Downregulation of dopamine D1-like receptor pathways of GABAergic interneurons in the anterior cingulate cortex of spontaneously hypertensive rats. Neuroscience 394: 267–285, 2018.
- Bymaster F, Katner J, Nelson D, Hemrick-Luecke S, Threlkeld P, Heiligenstein J, Morin M, Gehlert D, and Perry K. Atomoxetine increases extracellular levels of norepinephrine and dopamine in prefrontal cortex of rat a potential mechanism for efficacy in attention deficit/hyperactivity disorder. Neuropsychopharmacology 27: 699– 711, 2002.
- Zhou J. Norepinephine transporter inhibitors and their therapeutic potential. Drugs of the Future 29: 1235, 2004.
- Szopinska-Tokov J, Dam S, Naaijen J, Konstanti P, Rommelse N, Belzer C, Buitelaar J, Franke B, Bloemendaal M, Aarts E, Arias Vasquez A. Investigating the gut microbiota composition of individuals with attention-deficit/hyperactivity disorder and association with symptoms. Microorganisms 8: 406, 2020.
- Aarts E, Ederveen TH, Naaijen J, Zwiers MP, Boekhorst J, Timmerman HM, Smeekens SP, Netea MG, Buitelaar JK, Franke B, van Hijum SA, Arias Vasquez A. Gut microbiome in ADHD and its relation to neural reward anticipation. PLOS ONE 12,
- Zhang P, Fang H, Lou C, Ye S, Shen G, Chen S, Amin N, Botchway BO, Fang M. Enhanced glial reaction and altered neuronal nitric oxide synthase are implicated in attention deficit hyperactivity disorder. Frontiers in Cell and Developmental Biology 10,
- Lovell B, Moss M, Wetherell M. The psychosocial, endocrine and immune consequences of caring for a child with autism or ADHD. Psychoneuroendocrinology 37: 534–542, 2012.
- Varambally S, Hariprasad VR, Arasappa R, Srinath S, Gangadhar BN. Feasibility and efficacy of yoga as an add-on intervention in attention deficit-hyperactivity disorder: An exploratory study. Indian Journal of Psychiatry 55: 379, 2013.
- Converse AK, Barrett BP, Chewning BA, Wayne PM. Tai Chi training for attention deficit hyperactivity disorder: A feasibility trial in college students. Complementary Therapies in Medicine 53: 102538, 2020.
- Hemandez-Reif M, Field TM, and Thimas E. “Attention deficit hyperactivity disorder: benefits from tai chi,” J. Bodym. Mov. Ther, vol. 5, no. 2, pp. 120–123, 2001.
- Jeong HI, Ji E-S, Kim S-H, Kim T-W, Baek S-B, Choi SW. Treadmill exercise improves spatial learning ability by enhancing brain-derived neurotrophic factor expression in the attention-deficit/hyperactivity disorder rats. Journal of Exercise Rehabilitation 10: 162– 167, 2014.
- Fritz K, O’Connor P. Acute exercise improves mood and motivation in young men with ADHD symptoms. Medicine & Science in Sports & Exercise 48: 1153–1160, 2016.
- Abd El Baaki OM, Abd El Hamid ER, Zaki ST, Alwakkad AS, Sabry RN, Elsheikh EM. Diet modification impact on ADHD outcome. Bulletin of the National Research Centre 45, 2021.
- Sharif MR, Madani M, Tabatabaei F, and Tabatabaee Z. The Relationship between Serum Vitamin D Level and Attention Deficit Hyperactivity Disorder. Iranian journal of child neurology, 9(4), 48–53, 2015.
Figure
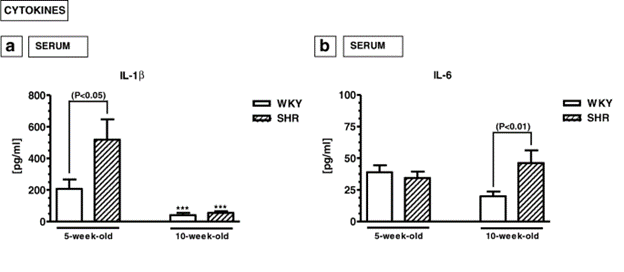 Figure 1. Adapted from Kozłowska A et al. (2019). 5-week-old (juvenile) and 10-weekold (mature) spontaneously hypertensive rats (SHRs, ADHD animal model) and Wistar
Kyoto rats (WKYs, control animals). Juvenile SHR rats express significantly higher levels of serum interleukin (IL)-1β compared to controls. Mature SHR rats express significantly higher levels of serum interleukin (IL)-6 compared to controls. Results are from ELISA experiments, and the units are pg/mL. P < 0.5 indicates significance.
Figure 1. Adapted from Kozłowska A et al. (2019). 5-week-old (juvenile) and 10-weekold (mature) spontaneously hypertensive rats (SHRs, ADHD animal model) and Wistar
Kyoto rats (WKYs, control animals). Juvenile SHR rats express significantly higher levels of serum interleukin (IL)-1β compared to controls. Mature SHR rats express significantly higher levels of serum interleukin (IL)-6 compared to controls. Results are from ELISA experiments, and the units are pg/mL. P < 0.5 indicates significance.